–What can genetic studies tell us about the risk of developing diabetes with cholesterol-lowering therapies?
This post was first published on MedPageToday and CardioBrief.org.
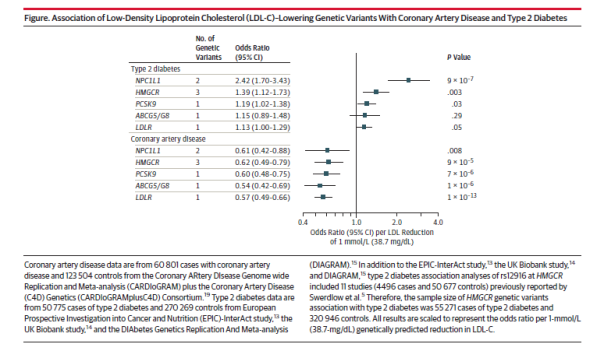
In a study published in the Journal of the American Medical Association, several LDL-lowering genetic variants were found to be associated with a reduced risk of coronary artery disease and an increased risk of type 2 diabetes. The study investigated LDL-lowering alleles in or near Niemann-Pick C1-Like 1 (NPC1L1), HMG-CoA reductase (HMGCR), PCSK9, ABCG5/G8, and low density lipoprotein receptor (LDLR). NPC1L1 is the target of ezetimibe, while HMGCR is the target of statins and PCSK9 is the target of PCSK9 inhibitors.
Luca Lotta, of the University of Cambridge, and colleagues conducted meta-analyses of genetic association studies, and included 50,775 individuals with type 2 diabetes and 270,269 controls and 60,801 individuals with CAD and 123,504 controls.
The study found that for a 38.7 mg/dL reduction in LDL-cholesterol, the genetic variants were associated with a similar reduction in risk of coronary artery disease, with odds ratios ranging from 0.54 to 0.62. However, genetic variants at the NPC1L1 locus were associated with a higher risk of diabetes (odds ratio 2.42) as compared to controls than the HMGCR and PCSK9 genetic variants (odd ratios of 1.39 and 1.19, respectively). The type 2 diabetes findings for NPC1L1 and HMGCR were highly significant (p = 9 x 107 and p = .003, respectively), but the p value for the type 2 diabetes finding for the PCSK9 variants was .03. The associations with type 2 diabetes for ABCG5/G8 and LDLR were not significant.
Treatment with statins is known to be associated with a higher incidence of new-onset diabetes, as is treatment with niacin, but the effect of ezetimibe and PCSK9 inhibitors on new-onset diabetes is unclear. An analysis of the IMPROVE-IT trial showed a small increase in new-onset diabetes in the ezetimibe group, but the difference was not statistically significant. The published data for the PCSK9 inhibitors have not shown statistically significant increases in blood sugar or new-onset diabetes (see here and here), but much more data will be available when the PCSK9 inhibitor outcomes trials are completed, starting next year.
One reason to wonder why PCSK9 inhibitors might increase blood sugar is that both statins and PCSK9 inhibitors have mechanisms of action that involve the removal of LDL from the bloodstream through upregulation of the LDL receptors. A recent study showed that patients with familial hypercholesterolemia, a disease that involves dysfunction of the LDL receptors, have a lower prevalence of type 2 diabetes as compared to their unaffected relatives. The study suggests that LDL receptor function may be involved in glucose homeostasis. I asked several experts in clinical trials or cardiovascular genetics to comment by email.
Sanjay Kaul, MD, of Cedars Sinai Medical Center in Los Angeles, sent the following comment by email:
The association of LDL-lowering alleles with CV risk is consistent across the 5 alleles. However, the association of LDL-lowering alleles with risk of T2DM is confined to NPC1L1 (large effect size, HR 2.4 and statistically robust p value) and to a lesser extent to HMGCR (HR 1.4, p = 0.003). This finding suggests an increased risk of incident diabetes with ezetimibe that targets NPC1L1. However, the incidence of new onset DM (defined as initiation of anti-diabetic medication during trial or two consecutive fasting glucose ≥126 mg/dL) in IMPROVE-IT trial was 720/5297 (13.6%) in EZ/SV vs. 694/5341 (13.0%) in SV, HR 1.04 95% CI (0.94, 1.15). The additional LDL lowering with ezetimibe was approximately 16 mg/dL which translates into a HR of 1.10 per mmol/L LDL lowering (1.04/16) x 38.7). This is considerably lower than the HR of 2.4 observed in the gene association study. Of course the median exposure in IMPROVE-IT was only 7 years when about 42% of subjects had discontinued treatment compared with the lifetime exposure in the gene association study. One would need a larger data set (meta-analysis of SHARP, SEAS, IMPROVE-IT, ARBITER-6, etc.) to better characterize the risk of incident T2DM. Even if we assume the association to be causal, remember the treatment effect in IMPROVE-IT was exclusively confined to the diabetic cohort who comprised 27% of the overall cohort (HR 0.86, 95% CI 0.78, 0.84 vs HR 0.98 for the non-diabetic cohort).
Joshua Knowles, MD, PhD, of Stanford University in California, sent the following comment:
This is an important paper by a very good group of investigators. The overall results of this Mendelian randomization study are not that surprising but are still very important, that there is an inverse relationship between LDL-C lowering genetic alleles and risk of type 2 diabetes.
There has been a lot of evidence emerging about this from the large statin trials to studies of [familial hypercholesterolemia (FH)] patients to prior Mendelian randomization studies.
The fact that they observe some heterogeneity of effect is interesting in that it might suggest that different ways of lowering LDL-C might result in different levels of risk for type 2 diabetes.
The overall effect they see for NPC1L1 genetic variants (a risk of 2.42 for type 2 diabetes for every 1 mmol/L reduction in LDL-C) suggests that this mechanism might theoretically be more potent for causing T2D risk.
However, in practice, ezetimibe does not lower LDL-C by 1 mmol/l but more like by ~0.5 mmol/L (or even less) so the actual effect size in ezetimibe trials (like IMPROVE-IT) will be less than 2.4 (probably more like 1.2). And in IMPROVE IT the effects might be masked to some extent as everyone was also on a statin and we don’t know if the effects would be additive.
The large scale PCKS9 trials will be revealing for their risk. Certainly these studies do not suggest that there will be a big effect which is good for the patients taking them now.
Please emphasize that overall message remains that for high risk patients (like FH) the beneficial effect of LDL-C lowering will greatly trump the increased risk of type 2 diabetes.
What is fascinating for me is we really have no idea whether the increased T2D risk is because the drugs decrease insulin secretion or increase insulin resistance. Knowing this will be critically important.
I am very interested in this topic and have a Doris Duke Clinical Investigator Grant to study it in a randomized trial. We will be measuring (with gold standard measures) insulin secretion and insulin resistance pre and post statin.
Remember that T2D is simply defined as an increase in blood glucose. These drugs seem to mostly push people that are ALMOST diabetic just over the threshold (see our recent paper published in the American Journal of Cardiology). Simply having an average blood glucose level go from 123 mg/dl to 127 mg/dl probably is not that important to a single person’s individual risk of downstream bad outcomes (though that person would go from being a pre-diabetic to a diabetic with that small change in blood glucose). What may be more important is HOW and WHY that blood glucose level rose. If there is not enough insulin being made, the treatment would potentially be different than if the body is not responding to insulin.
Another key message is to reemphasize the importance of exercise and maintenance of a healthy weight to potentially counteract the effect of these LDL-C lowering drugs on T2D. We should continue to advocate those important lifestyle choices for our patients. If you look at the data in [our paper] the risk of T2D with a statin is EXTREMELY low (3%) in those with normal fasting glucose and normal triglycerides (or weight) but very high in patients with pre-diabetes and high triglycerides (or overweight)– 23%!
I also received this comment from Daniel Swerdlow, MBBS, PhD, of Imperial College London:
This is a well-designed analysis that uses methods that are now established for using genetics to explore the effects of drug target modulation. The associations of the variants in NPC1L1 and PCSK9 on type 2 diabetes risk are not unexpected, as it appears from other large genetic analyses published recently that LDL-C lowering associates with higher diabetes risk, regardless of the mechanism through which this is achieved. This has been borne out in trials of statins and niacin, though the IMPROVE-IT trial of ezetimibe did not demonstrate an increased risk of diabetes in the treatment arm. The effect sizes in studies such as this are less informative than the direction of the effect, since direct comparison of the magnitudes of genetic effects and drug treatments is restricted by the differences in duration and potency of the two ‘interventions’. The biological analogy, however, allows the directions and scope of genetic associations to be interpreted as proxies for drug effects on the target encoded by the gene in question. The issue of new onset diabetes risk is pertinent for the PCSK9 inhibitors, and although analyses of trial data to-date has shown no association, they have been limited by duration of follow-up and sample size. The large phase 3 outcome trials are expected to focus carefully on diabetes risk with these new agents.
The over-riding message that analyses such as this in JAMA emphasize is that lipid-modifying treatments are only one part of cardiovascular risk reduction, and must be accompanied by lifestyle modification, such as appropriate diet and higher physical activity, in order to optimize risk reduction and mitigate against the small increase in diabetes risk that has been shown to be associated with some lipid-modifying drug treatments.





















